How to Improve Respiratory Training and Reduce Time-to-Floor

The COVID-19 pandemic has led to an increase in the demand for respiratory care training. As the widespread shortage of ventilators gained public awareness, hospitals and long-term care facilities also grappled with the shortage of healthcare personnel trained to operate them. For organizations training existing staff, new hires, and returning retirees, the challenge has become how to speed up the educational delivery model without sacrificing provider competence and patient safety.
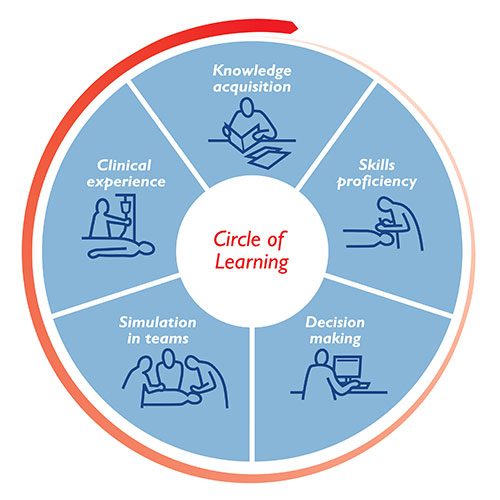
At Laerdal Medical, we encourage clients to adopt our Circle of Learning model as a means to achieve better training results and more competent healthcare professionals in a shorter timeframe. Using a "building block" approach, learners master each individual stage of learning before moving onto more complex concepts.
Traditionally, training begins with textbook reading, lectures, and other forms of didactic learning which require an educator’s time and expertise. A more efficient way to begin engaging learners is through eLearning.
Mechanical Ventilation E-learning can prepare learners for more comprehensive respiratory care training while providing flexibilty in when and where they complete the learning modules. While students are free to work at their own pace, clinical educators earn back time that would otherwise be spent lecturing and use automated data reports to quickly identify learners who are struggling.


The mastery of skills is essential to providing the best possible treatment to patients. For many respiratory therapists and technicians, skills training usually takes place at the bedside on a real patient. Unfortunately, treating respiratory patients who have tested positive for COVID-19 leaves little room for error.
The Laerdal Airway Management Trainer is a lifelike upper torso and head that can be used to simulate intubation, ventilation, and suction techniques. Learners gain realistic experience performing tasks that match their current stage of learning – without the risk of potential patient harm.
Critical-thinking and decision-making have always been important among healthcare providers, but this year these skills have become paramount. At times when hospitals are nearing maximum capacity and critically-ill patients with COVID-19 are multiplying, the ability to make a quick and accurate decision means the difference between a negative versus positive patient outcome.
TruVent, a virtual training solution, builds clinical competence and confidence to manage a patient on a ventilator. Educators can create clinically-accurate respiratory simulations that will display appropriate pressure, flow, and volume curves. By witnessing these changes in real-time, learners will develop the ability to recognize signs of respiratory distress and make rapid treatment decisions.


70% of patient harm is due to a breakdown in communication. Traditional training models fail to include communications and teamwork training. The Circle of Learning has an entire stage of learning dedicated to reducing human error in teams.
Consider the team dynamics involved when proning a patient with an average of six healthcare providers working in different disciplines. One provider’s wrong move or miscommunication can lead to drastic changes in the patient’s physiological state. Now consider the positive impact it can make if each of the six providers recently simulated a scenario requiring proning.
The ASL 5000™ Lung Solution can be used to run scenarios with a spontaneously breathing patient simulator supported on a ventilator. The ability to simulate any respiratory condition on any ventilator provides learners with the opportunity to work together as they would in a real patient case.
Respiratory therapists and technicians have not traditionally used simulation for clinical experience, but COVID-19 may change that. In 2015, the National Council of State Boards of Nursing (NCSBN) published a study supporting that high-quality simulation experiences could be substituted for up to 50% of traditional clinical hours. Over the past five years as the availability of clinical time has reduced, many states have adjusted their prelicensure requirements to allow for more simulation training.
The repeatability of scenarios run on a high-fidelity patient simulator allows for a more immersive and consistent training experience. Organizations can use simulation to standardize training among respiratory care practitioners and hold them accountable for the same standard of safe patient care.

The Circle of Learning approach challenges clinical educators to rethink how to effectively train healthcare providers. By using this model and the appropriate simulation solutions, organizations can foster safe respiratory caregivers while reducing their time to the floor.
Melden Sie sich für E-Mail-Updates von Laerdal Medical an. Wählen Sie Ihre Interessengebiete aus und erhalten Sie neue Fachinhalte, aktuelle Informationen, Veranstaltungshinweise und mehr.

