
Elvytyskoulutus
Koulutusratkaisuja, joiden tarkoitus on auttaa parantamaan mahdollisuutta selvitä sydänpysähdyksestä.


Tiedämme, että hyvä PPE mahdollistaa korkeamman eloonjäämisprosentin, ja pisteytyksen tarkoituksena on antaa käsitys siitä, miten hyvä suoritus todella on potilaalle.
Laerdalin PPE-pisteytysalgoritmi antaa oppijoille tarkan pistemäärän heidän elvytyssuorituksestaan ja ohjaa heitä antamaan entistä parempaa painelu-puhalluselvytystä. Miten voit ymmärtää pisteiden takana olevat numerot?
Miksi oppija 2 on saanut paremman pistemäärän,
vaikka oppijalla 1 oli parempi painelusyvyys?
Oppija 1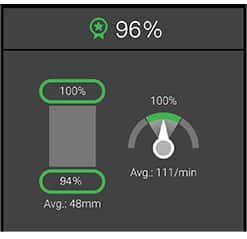
Oppija 2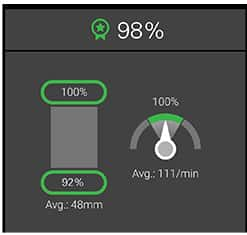
Nopea vastaus on, että huippuluvut, kokonaispistemäärät 96 % ja 98 % ovat ei-binäärilukuja. Tämä luku lasketaan kaikista QCPR-algoritmia ohjaavista komponenteista. Yllä olevien kuvien kolme muuta numeroa ovat binäärilukuja.
Binääripistemäärä laskee vain sen, kuinka monta kertaa oppijan painallukset ovat suositeltujen ohjeiden mukaisia, kun taas ei-binäärinen algoritmi mittaa, kuinka lähellä oppija on absoluuttista suoritusta.
Ylläoleva esimerkki näyttää, että oppijan 2 rintakehän paineluista 92 % oli syvyydeltään suositusten mukaisesti 5-6 cm. Syy, miksi hänen kokonaispistemääränsä on korkeampi kuin oppijalla 1 johtuu siitä, että "väärien" paineluiden syvyys oli lähempänä suositusten mukasta arvoa. Tästä lisää myöhemmin.
Kokonaispistemäärä on yksinkertainen tapa esittää se, miten hyvä elvytyssuoritus oli, mutta matematiikka pisteytyksen takana voi olla mutkikas. Tällä sivulla kerromme pistelaskun periaatteet, ja miten voit parantaa elvytyskoulutusta.
We know good CPR gives higher survival rates, and the idea about scoring is to reflect how good the performance really is for the patient.
Previously, CPR feedback has been given with a strict approved/non-approved result. Over the last 10 years, Laerdal and our partners have created an algorithm providing a more detailed and granular CPR score. Let’s illustrate with an example:
Julie is an emergency nurse in a UK hospital. She is physically fit, and able to provide solid depth of more than 50mm in every compression - all fully released and with absolutely no interruptions. She is one of the best CPR performers we’ve ever seen. Still, after the session, the binary CPR feedback said she had failed. Why?
The rate of her compressions were a consistent 122 compressions per minute. Clinically superb, but just a tiny bit outside of the magic 100-120-limit in the guidelines. Was it fair to tell her she failed? No. If your life was on the line, you’d want Julie to perform CPR on you.
We saw these results all the time when using the old, binary scoring, and this is one of the reasons we made a new algorithm for scoring CPR.
While other providers of CPR scoring only use binary numbers, Laerdal uses a non-binary approach to present a more realistic and lifesaving performance review. The simple reason is that while both 49 mm and 25 mm compression depth is outside of the guideline threshold, 49 is undoubtedly, and by far, a much more desired performance.
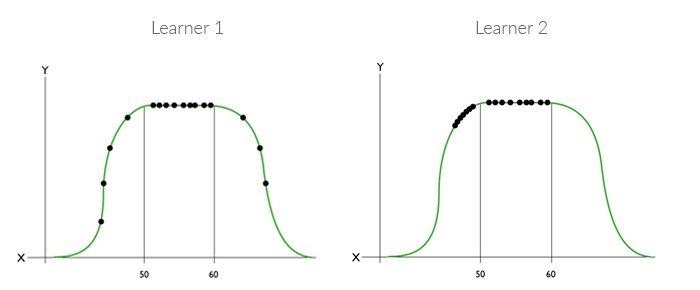
Fig 1. Non-binary scoring.
Learner 1 and 2 have equal amount of compressions inside and outside of the guideline threshold. But Learner 2 get the higher score since compressions outside the thresholds are closer to the guideline. The same principle is used on all other CPR skills. (figure not to scale, for illustrative purposes only)
The algorithm which makes up the QCPR score is made by Laerdal Medical in close collaboration with members of the AHA ECC Subcommittees and co-authors of the 2013 AHA Consensus Statement on CPR Quality. Based on input from these specialist members, we created mathematical models for each sub-skill in CPR performance, like compression depth, leaning, ventilation volume, etc.
Each compression and ventilation are tracked and scored individually and summed up in the overall score. Even though numbers like average rate can be interesting, averages are not used to calculate the overall score. Similarly, the binary numbers do not affect the score calculation directly.
Subtractive scoring model
The scoring algorithm use a subtractive scoring model where we start off on a perfect score and, if the learners do something wrong, the score is reduced. If you are within the guidelines you will always get a 100% score. If you deviate, the score is reduced.
Plotted along an S-curve, we can see that small deviations give small reductions in the overall score, while large deviations result in large reductions in CPR scores:
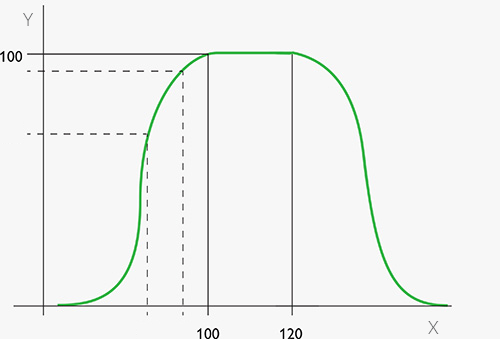
Fig.2 : Compression rate on the x-axis, and score on the y-axis.
We see that the CPR score deteriorates quickly on both sides of the guideline thresholds. (graph not to scale, for illustrative purposes only)
A popular feature of our QCPR manikins is the QCPR race where up to six learners can participate in a race to see which one performs the best CPR.
Sometimes we see that while one participant achieves the best score on binary sub-metrics (like adequate depth percentage), another participant will be crowned the winner of the race. The binary sub-metrics (like percentage of adequate depth) will not always help explain the CPR score.
Two learner perform 100 compressions. Learner 2 gets a better overall score than learner 1, even though learner 1 had better compression depth if you only look at the binary metrics.
The reason is that learner 2 was closer to the guidelines during the 10 compressions that were not fully "adequate", and learner 1 was very far away from the guidelines during the 8 compressions that were not "adequate".
In another example, both learners provide too much air in ventilation and miss the ventilation sub-metric.
Let's say learner 2 gave 610 ml of air (which is clinically OK) and learner 1 provided 2000ml of air, which indeed can compromise the clinical outcome. In binary terms, these results are the same, simply "not adequate". However, in clinical terms, and therefore also in scoring terms, they are very different. Learner 2 was much closer to the guidelines and receives a higher score.
Sometimes - especially for 'Compressions Only' sessions - the total score is unexpectedly low, even though compression rate, depth, and release are all perfect (see image below).
The score reduction for many of those sessions comes from the chest compression fraction. If your compressions are interrupted, there will be a reduction in the score - longer interruptions give larger score reductions.
Also worth noting, if you are running a ”Compression only” sessions, the expected chest compression fraction is 100%, as you have no good reasons to stop the compressions. So, if there are interruptions, the score is reduced rather strictly.
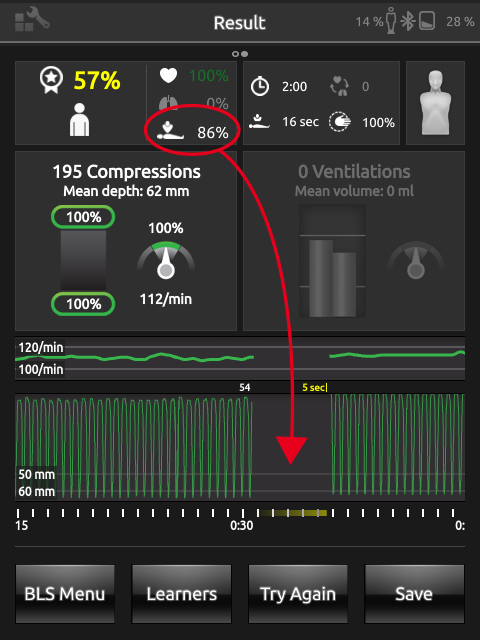
Illustration, Compression only session: Rate, depth, and release are all perfect. However, the total score is unexpectedly low. The culprit is the chest compression fraction parameter.
The number of parameters scored depends on which manikin or simulator you use, and which software or application you use.
10 parameters used to calculate QCPR score: