As our global population becomes increasingly more diverse, so too does the patient population. And, this should affect how healthcare professionals train for their roles.
There has been a significant focus on promoting diversity, equity, and inclusion in healthcare education with the intention of acknowledging health disparities and improving the quality of care and health outcomes for groups outside of dominant power structures.
The problem is known – disparities exist across dimensions of race, ethnicity, gender, age, education level, and geographic location. The solutions can seem far less certain.
There are societal, structural, and personal biases that negatively impact health disparities globally. Where we seek to focus is on the training of healthcare professionals and how stronger training methods can develop more culturally-competent and cognizant providers.
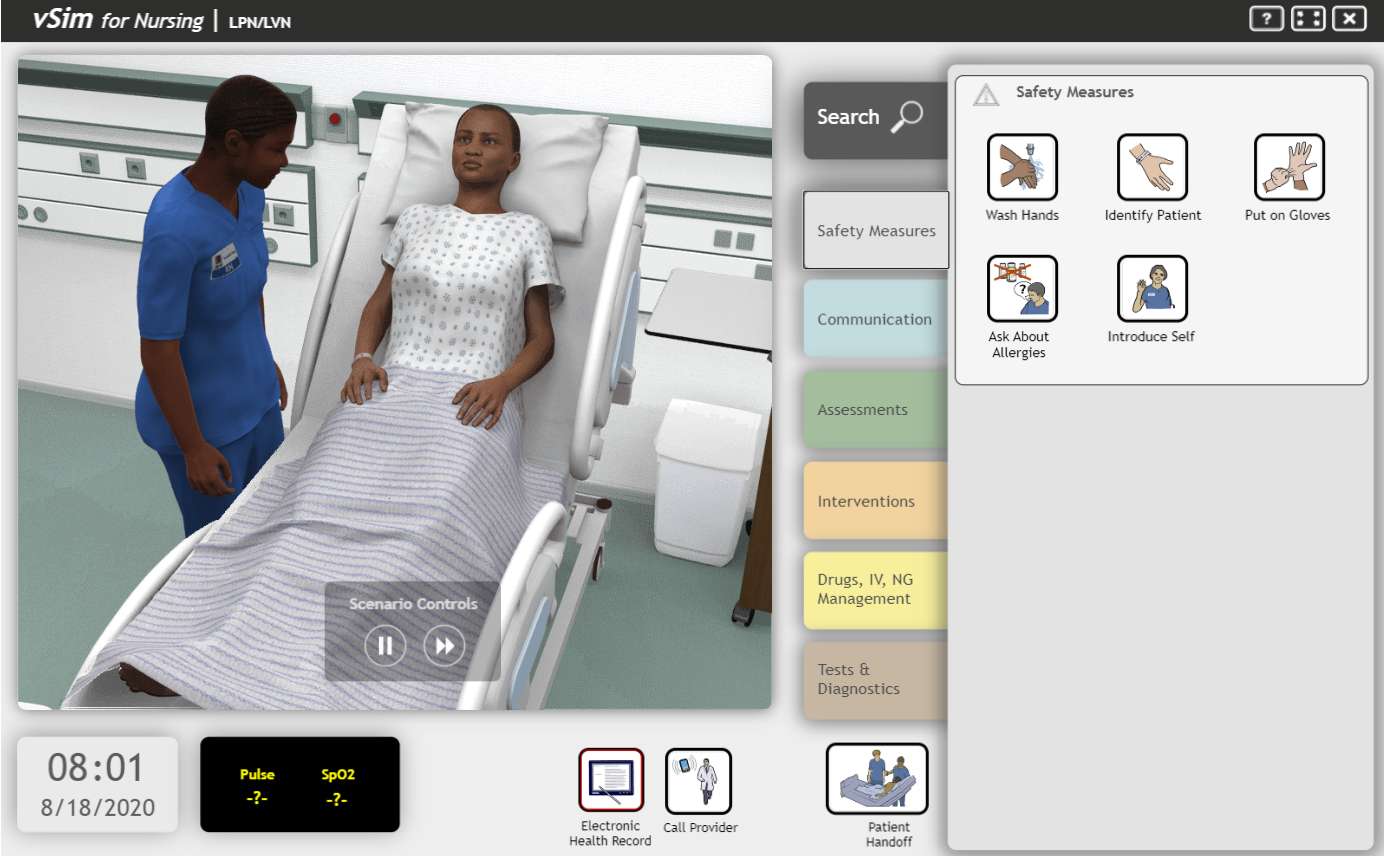
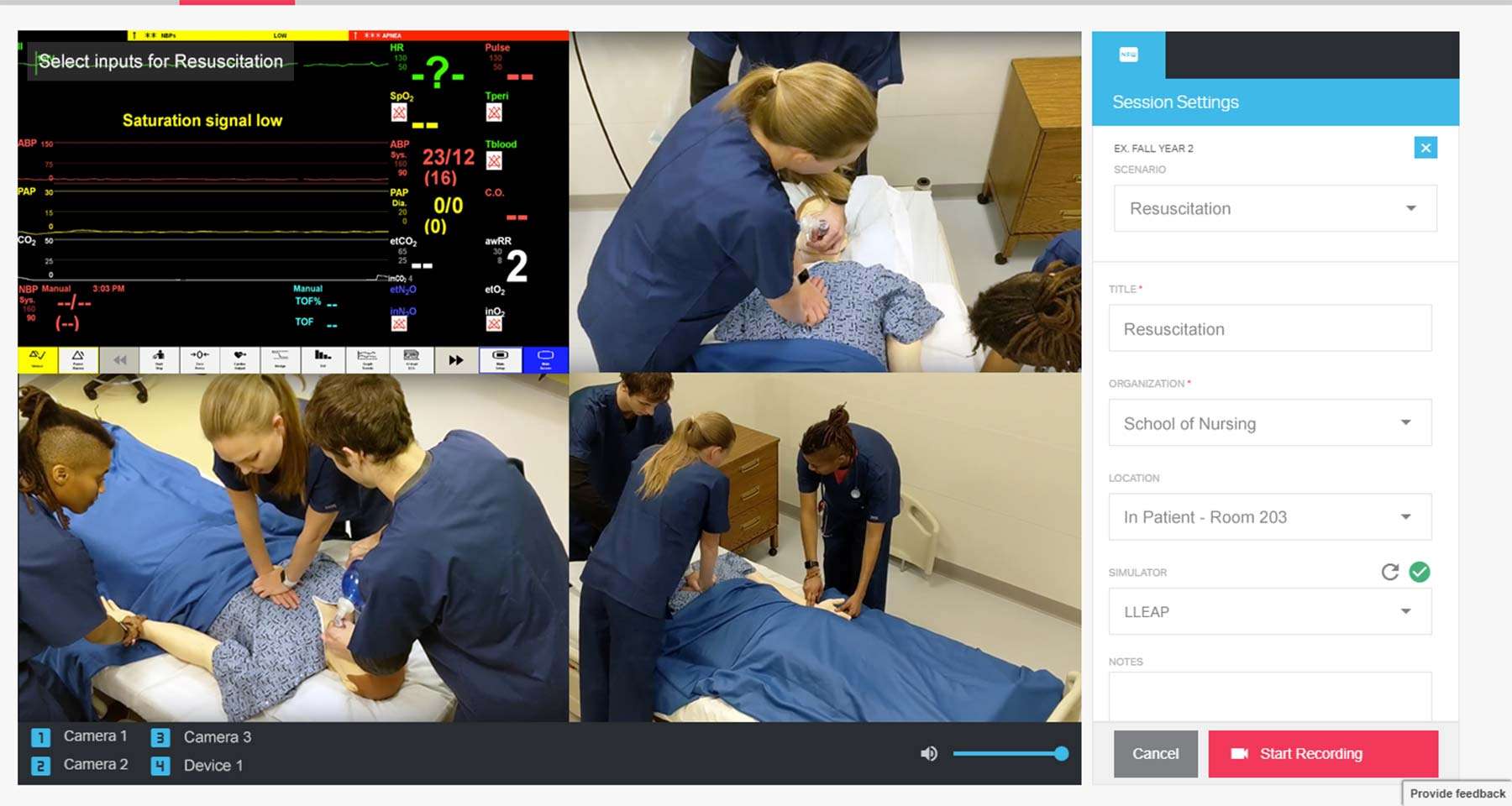
There are many benefits of using simulation to train healthcare providers and providers-in-training, including, making knowledge come alive, increasing clinical understanding, boosting confidence to treat acute cases, and many more.
In this article, we discuss how simulation can help to reduce implicit bias and mitigate risk to patients of diverse backgrounds. This article includes example scenario cases and helpful tools to make or propose an educational shift in your organization with the goal of guiding more culturally-diverse learning experiences and influence safer, more equitable healthcare.