Naarmate de wereldbevolking meer gediversifieerd raakt, wordt ook de patiëntenpopulatie alsmaar diverser.Dit zou zich moeten uiten in de manier waarop gezondheidsprofessionals worden opgeleid voor hun functie.
Er worden veel inspanningen geleverd om zowel diversiteit, gelijkheid als inclusie te integreren in het zorgonderwijs, zodat ongelijkheden in de gezondheidszorg kunnen worden aangepakt en de kwaliteit van de zorg en de gezondheidsresultaten van minderheidsgroepen kunnen worden verbeterd.
Het is een gekend probleem – ongelijkheden komen voor ongeacht ras, etniciteit, geslacht, leeftijd, opleidingsniveau en geografische locatie.De oplossingen zijn niet altijd even vanzelfsprekend.
Wereldwijde maatschappelijke, structurele en persoonlijke vooroordelen hebben een negatieve invloed op verschillen in de gezondheidszorg.We richten ons op de training van zorgverleners om een meer cultureel verantwoorde en bewuste zorgcultuur te bewerkstelligen.
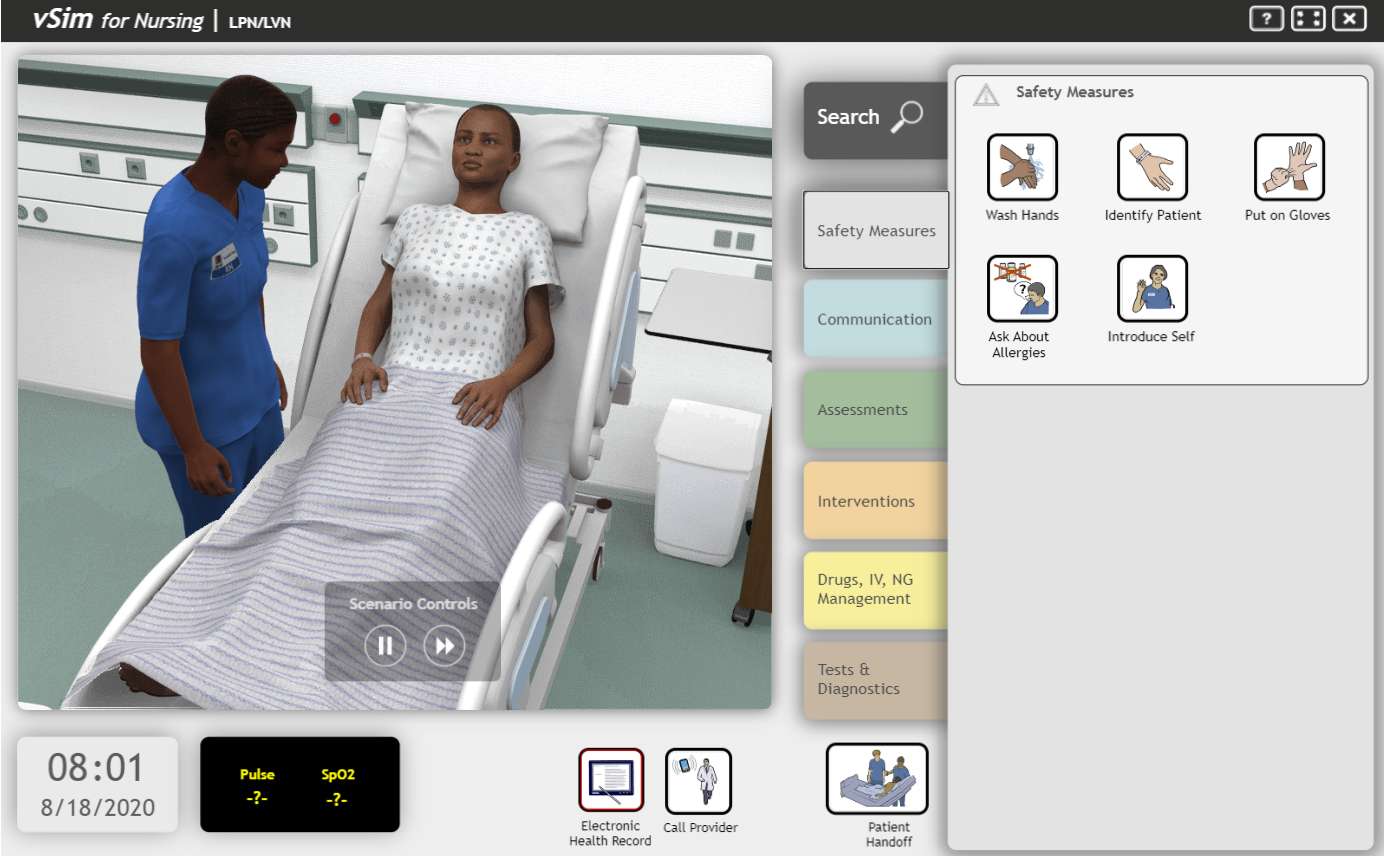
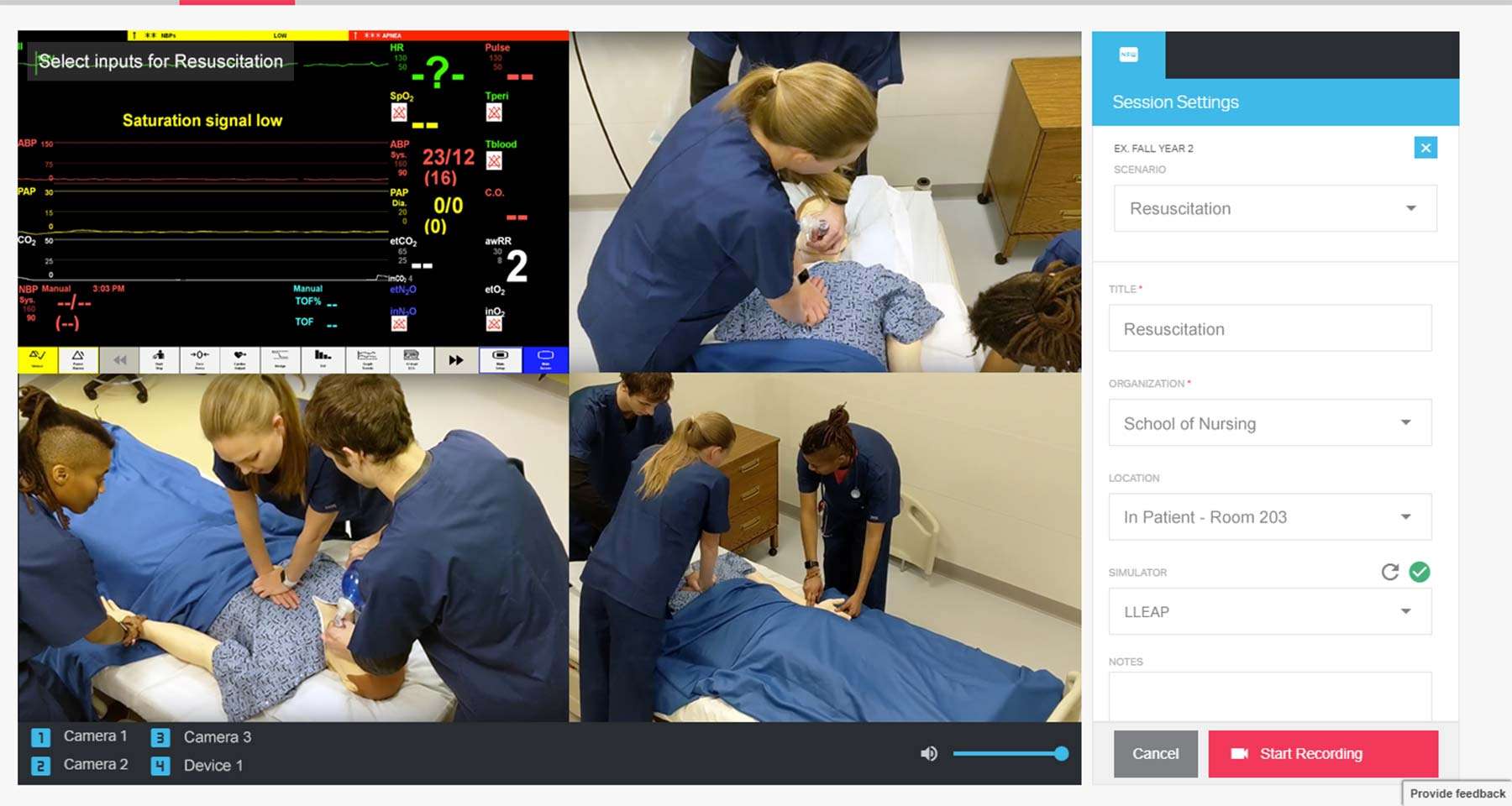
De toepassing van simulatietraining voor zorgverleners en zorgverleners in opleiding heeft vele voordelen, zoals het opdoen van levensechte kennis, toegenomen klinisch inzicht, meer zelfvertrouwen om acute noodgevallen te behandelen, en nog veel meer.
In dit artikel bespreken we hoe simulatie kan bijdragen aan het terugdringen van impliciete vooringenomenheid en aan het beperken van de risico's voor patiënten met diverse achtergronden.Dit artikel omvat praktijkvoorbeelden en nuttige hulpmiddelen om de opleidingen binnen uw organisatie te herzien of uit te breiden, om een meer cultureel gediversifieerde leeromgeving te bevorderen en zo meer gelijkwaardige en rechtvaardige gezondheidszorg te bewerkstelligen.