Hur man minskar OB/GYN-mål om felbehandling
En banbrytande studie visar hur patientsimulering kan vara en gynekologs bästa försvar

En banbrytande studie visar hur patientsimulering kan vara en gynekologs bästa försvar
En studie från 2021 publicerad i Obstetrics & Gynecology avslöjade några övertygande resultat för obstetriker/gynekologer (OB/GYNs) – men även för de som arbetar med riskhantering. Studien, “Association of Simulation Training with Rates of Medical Malpractice Claims Among Obstetrician-Gynecologists,” kan vara banbrytande. Den visade att simulering träning avsevärt minskade frekvensen av anspråk på felbehandling för OB/GYNs.1
I den här artikeln ger vi dig några viktiga insikter från studien, samt lite eget innehåll och forskning med anknytning till ämnet maternella resultat.
Även om minskade krav på felbehandling användes som ett mått, handlar studien i slutändan om att förbättra patientresultat.
Studien understryker att i USA beräknas förlossningsrelaterade negativa händelser inträffa vid mellan 2% och 16% av alla förlossningar. En analys fann att 40,5% av de negativa händelserna kunde ha förhindrats.2
Mödradödligheten i USA har fortsatt att öka under de senaste decennierna.3 Ny data visar att mödradödligheten år 2021 var 32,9 dödsfall per 100 000 levande födda, jämfört med 23,8 år 2020.4 Detta innebär en ökning på 38% av mödradödsfallen. Siffran för svarta kvinnor var 2,6 gånger högre än siffran för icke-spansktalande vita kvinnor.
Dessa alarmerande siffror väcker oro inte bara för patientsäkerheten, utan även för juridisk ansvarighet. Obstetriker och gynekologer har en av de högsta försäkringspremierna för felbehandling inom läkaryrken,5 och 79% av obstetriker och gynekologer har varit involverade i en rättsprocess gällande felbehandling.6
Oavsett din koppling till förlossning och barnfödslar bekräftar data att åtgärder för att påverka dessa siffror borde vara en prioritet.
Den retrospektiva studien leddes av läkare och personal kopplade till fyra institutioner: Center for Medical Simulation, Brigham and Women's Hospital, Harvard Medical School och CRICO/Risk Management Foundation vid Harvard Medical Institutions.7 De undersökte prestationerna hos 292 OB/GYN-läkare, som alla var försäkrade av samma försäkringsbolag och alla deltog i en eller flera simulationsutbildningar från 2002 till 2019. Utbildningarna omfattade lågfrekventa, högintensiva obstetriska scenarier och fokuserade på teamarbete, kommunikation och organisationskultur. Varje utbildning följdes omedelbart av en feedbackgenomgång.
Vad studien avslöjade är att simulationsutbildning resulterade i en nästan 50-procentig minskning av antalet vårdslöshetskrav.
Vad studien också avslöjade är att deltagande i mer än en simulationsutbildning var associerat med en större minskning av antalet krav. Läkare som deltog i tre eller fler utbildningar hade en signifikant lägre frekvens av krav efter utbildning jämfört med läkare som deltog i en enstaka utbildning.
Forskning har tidigare gjorts inom detta område men har inte blivit lika uppmärksammad.
År 2012 publicerade Premier Hospital-nätverket en liknande studie baserad på 14 sjukhus som deltog i Premier Perinatal Safety Initiative, som syftade till att utbilda OB/GYN-läkare och bistå personal vid hantering av perinatala nödsituationer. De 14 sjukhusen använde simulering som en träningsmetod. Resultaten visade att OB-fordringar per förlossning vid de 13 sjukhusen minskade med 37%.9, 10
Att mäta effektiviteten av ett simulationsprogram kan vara en utmaning. I många studier används Likert-skalor för att mäta huruvida deltagaren kände att utbildningen var värdefull eller tror att deras färdigheter har förbättrats, jämfört med att titta på effekten på kliniska resultat.11 Likert-skalor presenterar deltagare med ett påstående och ber dem att betygsätta i vilken utsträckning de håller med om det, med värden som sträcker sig från "instämmer helt" till "neutral" till "instämmer inte alls."12
I denna studie tar felbehandlingsanmälningar i stort sett Likert-skalans eller andra måttens plats. Studien pekar på att anmälningsfrekvens är en objektiv, påtaglig indikator på framgång. Den stora försäkringsbolaget CRICO övervakade insamlingen av anmälningsdata för att säkerställa opartiskhet och tillförlitlighet.
När det gäller vilken påverkan simulering kan ha på ett sjukhus ekonomiska resultat, visar denna studie hur simulering kan löna sig.
Författarna till studien bekräftade vad experter har känt till under en tid: färdigheterna som förvärvades under simuleringsträningarna – nämligen effektivt teamarbete i situationer med hög akuitet – bidrog till att främja säkrare vård, vilket ledde till färre negativa utfall som potentiellt kunde bli senare rättstvister.13
Oro över kommunikation och samarbete och hur de kan påverka patientresultat går tillbaka så långt som till Institute of Medicine’s berömda rapport, To Err Is Human, som publicerades 1999. När man ser på de bakomliggande orsakerna till negativa patienthändelser är kommunikations- och samarbetsproblem en gemensam nämnare.
Det fanns en tid då kommunikations- och samarbetsfärdigheter ansågs vara separata från kliniska färdigheter. Idag anses de vara en integrerad del av leveransen av kliniska färdigheter och patientsäkerhet.
Över 50 % av den genomsnittliga sjukhusets budget för riskhantering spenderas på förlossning.18 De enorma kostnaderna för ansvarsförsäkring har fått sjukhus att söka alternativ. En studie utförd av American Society of Healthcare Risk Management fann att 80 % av sjukhusens riskhanterare självförsäkrar sina läkare.19 Allt detta pekar tillbaka på riskerna som är förknippade med förlossning och de potentiella konsekvenserna för patienter – konsekvenser som experter är överens om är förhindringsbara i många fall.
Med de stigande mödradödlighetstalen är Laerdal engagerat i att hjälpa till att vända denna trend.
Laerdals uppdrag är att hjälpa till att rädda liv. Vi strävar efter det uppdraget genom att hjälpa organisationer som din att använda simulering för att utbilda och träna er personal för att ge optimal vård. Vårt mål är att rädda ytterligare 1 miljon liv per år före år 2030. Vi söker specifika områden inom sjukvården där behovet är avgörande, med förlossning som för närvarande är ett av de främsta.
Nedan hittar du en mängd resurser som hjälper dig komma igång med att använda simulering för att förbättra säkerheten för mödrar samtidigt som ansvaret minskas. Och om du vill prata med en representant från Laerdal, fyll gärna i formuläret nedan.




pdf | 0.99 MB
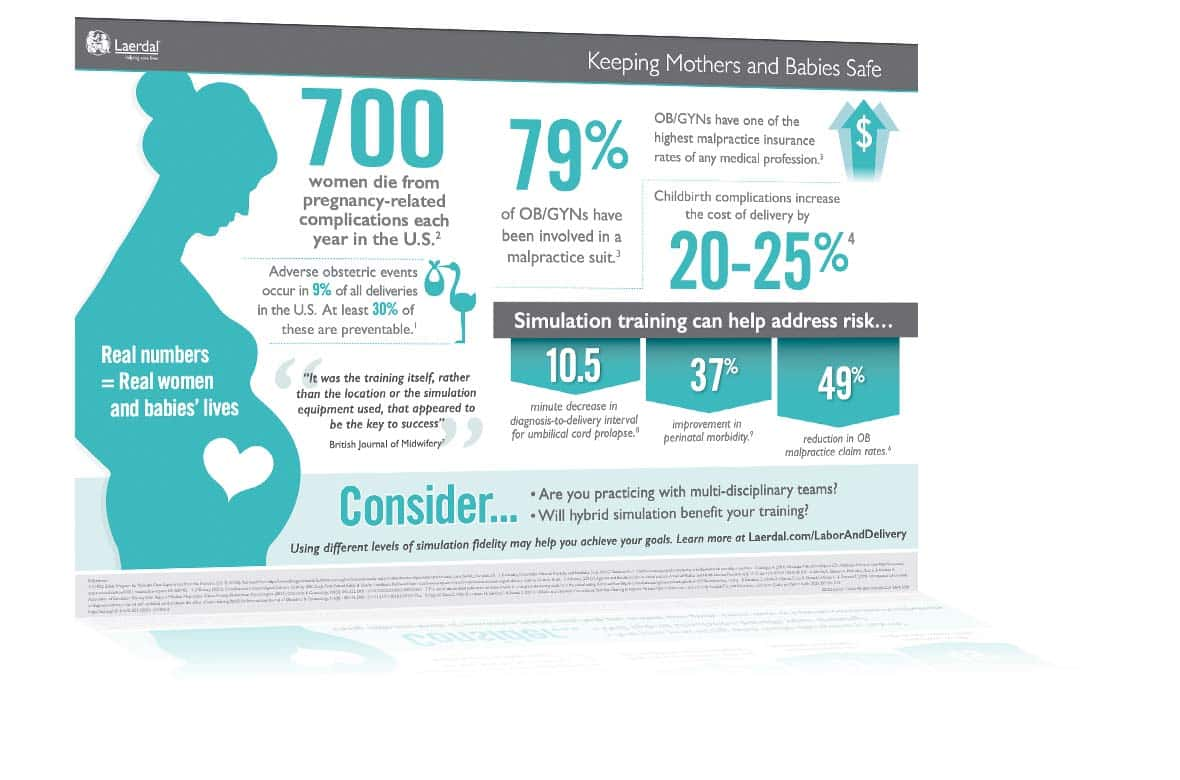
One of the most important objectives during labor and delivery is recognizing the potential risks to the mother and baby. Learn more with this free infographic.